Doctors perform both open and laparoscopic hernia repair based on what is best for the patient.
Book a Consultation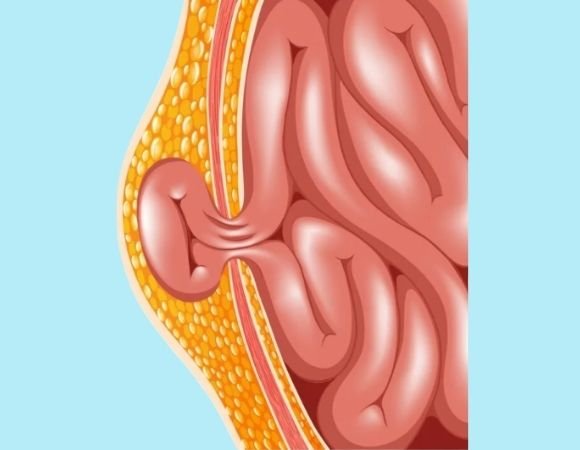
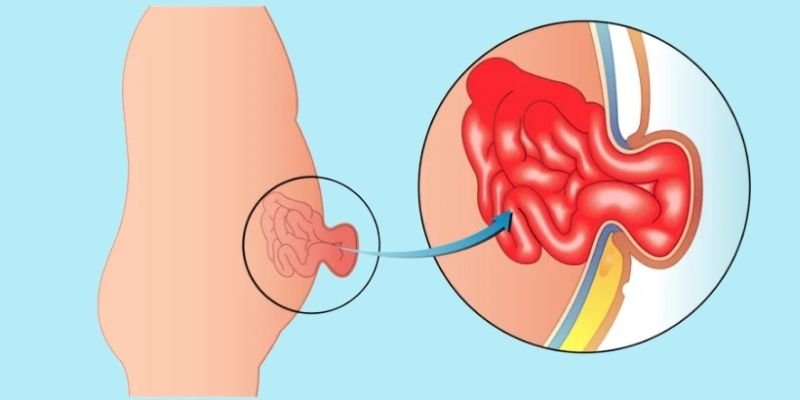
A hernia occurs when an internal portion of the body, such as the intestine, pushes through a weakened section of the muscle or tissue wall. Hernias are a common disease that affects both men and women, and their kind and severity vary greatly. A hernia does not get better over time, nor will it go away.
Hernias of the abdominal wall
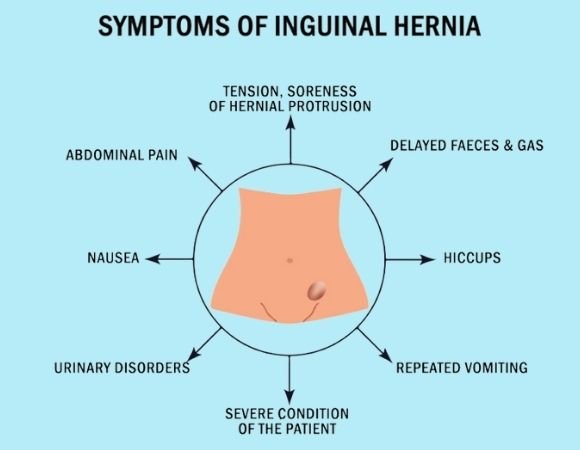
The symptoms of a hernia depend on its location and severity. Common signs include:
If the hernia becomes incarcerated (trapped) or strangulated (cutting off blood supply), it requires emergency surgery. In such cases, symptoms include:
Most inguinal hernias occur in men, and a small percentage of women develop inguinal hernias. The reason for the much higher prevalence in men relates to significant anatomical and embryologic differences. They are of 2 types, direct & indirect. When women develop inguinal hernias, it is almost always of the indirect variety.
The formation mechanism is different, but the end result is the same lining sliding alongside a uterine ligament that traverses the inguinal canal and anchors into the pubic bone. Another factor contributing to a higher male prevalence is significant differences in boney pelvis anatomy between sexes. The inguinal floor in males is generally broader and subjected to internal forces at higher pressures. This promotes gradual weakening of the floor and eventual eventration or bowing outward of the muscular floor. This type of hernia has been referred to as a direct inguinal hernia. This type of inguinal hernia is thought to develop due to “wear and tear”.
A hernia occurs when there is a hole in the muscles of the abdominal wall, allowing a loop of intestine or abdominal tissue to push through the muscle layer. A ventral hernia is a hernia that occurs at any location along the midline (vertical center) of the abdomen wall.
