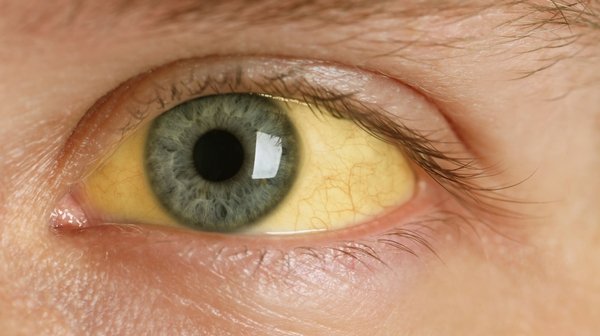
Jaundice - yellow discolouration of the skin or whites of the eyes - combined with abdominal pain is always a combination requiring urgent medical evaluation. The most common cause in India is obstructive jaundice from bile duct stones. When fever is also present (Charcot's triad), cholangitis is a life-threatening emergency. Early diagnosis and treatment significantly improve outcomes.
Quick Answers
Jaundice + Fever + Right Upper Pain = CHOLANGITIS - Go to Hospital Immediately
- Cholangitis is a life-threatening bile duct infection requiring urgent ERCP and IV antibiotics
- Mortality increases with each hour of delay to bile duct decompression
- Do not take antibiotics at home and wait - bile duct drainage is the essential treatment
Causes of Jaundice with Abdominal Pain
| Cause | Pattern | Key Feature | Management |
|---|---|---|---|
| CBD stones (Choledocholithiasis) | Right upper pain + jaundice; may have prior biliary colic history | Dilated bile duct on ultrasound; stones on MRCP; elevated bilirubin and ALP | ERCP for stone removal; then cholecystectomy |
| Cholangitis | Charcot's triad: fever + right upper pain + jaundice | Fever, rigors, altered consciousness in severe cases; urgent ERCP mandatory | IV antibiotics + urgent ERCP bile duct drainage |
| Cholangiocarcinoma (bile duct cancer) | Progressive painless jaundice, then dull right upper pain | Weight loss, pruritus; Klatskin tumour at bile duct bifurcation; MRCP + CT staging | Surgery (whipple or liver resection); stenting for palliation |
| Pancreatic cancer (head) | Progressive painless jaundice initially; back pain later | Weight loss, clay-coloured stool, dark urine; mass in pancreatic head on CT | Surgery (Whipple procedure) for resectable; stenting for palliation |
| Acute hepatitis (A, B, E) | Jaundice with diffuse upper abdominal ache, nausea, fever | Very high liver enzymes (AST, ALT); hepatitis serology confirms type; usually self-limiting | Supportive - rest, hydration; antivirals for hepatitis B in acute severe cases |
The key distinction is whether jaundice is obstructive (bile duct blocked - bile duct stones, cancer) or hepatocellular (liver cell damage - hepatitis). Obstructive jaundice shows elevated ALP and GGT predominantly; hepatocellular jaundice shows very elevated AST and ALT. Blood tests distinguish them quickly.
Investigations
- Blood tests - first line: Serum bilirubin (total, direct, indirect), liver enzymes (AST, ALT, ALP, GGT), full blood count, coagulation profile, hepatitis serology if viral hepatitis suspected
- Ultrasound abdomen: Identifies gallstones, CBD dilatation (suggests obstruction), liver size and texture, biliary tree
- MRCP: Non-invasive detailed imaging of the bile ducts - identifies CBD stones, strictures, tumours, level of obstruction
- ERCP: Diagnostic and therapeutic - removes CBD stones, allows brushings for cytology (cancer diagnosis), and places stents for palliation
- CT scan: For pancreatic and biliary malignancy staging
Treatment
CBD stones
ERCP (endoscopic sphincterotomy + stone extraction) - removes stones from the bile duct. Followed by laparoscopic cholecystectomy to prevent recurrence. Highly effective and safe in experienced hands.
Cholangitis
IV antibiotics immediately. IV fluids. Urgent ERCP within 12-24 hours for bile duct decompression. High-dependency monitoring. Followed by cholecystectomy once infection settles.
Biliary or pancreatic malignancy
Surgical resection for localised disease. Biliary stenting (endoscopic or percutaneous) for palliation of obstructive jaundice in unresectable cases. Multidisciplinary oncology team management.
Hepatitis
Supportive treatment. Hepatology specialist involvement. Antivirals for hepatitis B. Avoid hepatotoxic medications. Vaccination prevention for hepatitis A and B.
Frequently Asked Questions
This Symptom in India
Key India-specific factors
- Obstructive jaundice from CBD stones is one of the most common causes of jaundice presenting to surgical hospitals in India - almost always secondary to gallstone disease
- Cholangitis carries high mortality in India due to late presentation - many patients come to hospital after 2-3 days of fever and jaundice, having taken home antibiotics, by which time severe sepsis may be established
- Hepatitis A and E are common causes of jaundice with abdominal pain in India - particularly after contaminated water or food exposure, especially in monsoon season and in areas with poor water sanitation
- Gallbladder and bile duct cancer (cholangiocarcinoma) is unfortunately often diagnosed at an advanced stage in India due to late presentation with jaundice
Seek Care in Vadodara
Jaundice with abdominal pain - urgent evaluation at Sterling Hospital, Vadodara. Dr Samir Contractor provides ERCP, laparoscopic surgery, and biliary management for all causes of obstructive jaundice.
Desi Patient Questions
Ha - turant javo. Jaundice + pain = bile duct obstruction most likely, possibly cholangitis jyaré fever pan hoy. Blood tests + ultrasound + MRCP confirm karshe. ERCP thi bile duct stones remove thay chhe most cases ma. Delay nathi karvanu.
Jaundice during: avoid alcohol bilkul, oily/fatty food ochha karo, bland diet lo - khichdi, dal, sabzi without oil. However - dietary change is supportive, not treatment. Jaundice nu cause identify karvu zaruri chhe - ultrasound, blood tests, ane specialist evaluation first priority chhe.
Jaundice with Abdominal Pain? Get Urgent Evaluation in Vadodara
ERCP, biliary drainage, and laparoscopic surgery - all at Sterling Hospital, Vadodara under Dr Samir Contractor's care.