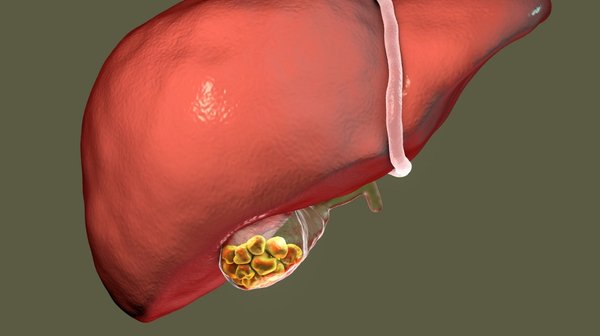
Gallstones are one of the most common surgical conditions in India, particularly among women aged 30-55. They form inside the gallbladder from bile components and range from tiny crystals to large stones. Most are asymptomatic. When symptomatic - producing right upper abdominal pain after fatty food - laparoscopic cholecystectomy provides a definitive, permanent cure.
Quick Answers
Gallstones affect approximately 10-15% of the Indian adult population, with women being affected 2-3 times more frequently than men. They are the leading cause of surgical hospitalisation related to the digestive system in India. Understanding gallstone disease - its types, natural history, complications, and treatment - is essential for any Indian patient receiving a first ultrasound showing gallstones.
Types of Gallstones
Cholesterol (80%)
- Most common type in India
- Yellow-green, waxy
- From supersaturated bile cholesterol
- Associated with obesity, high-fat diet, female sex
- May be dissolved by UDCA (slowly)
- Laparoscopy is definitive
Pigment (15%)
- From excess bilirubin
- Black or brown
- Associated with haemolytic anaemia, cirrhosis
- Cannot be dissolved - surgery needed
- Common in younger patients with sickle cell / thalassaemia
Mixed (5%)
- Combination of cholesterol and bilirubin
- Multiple, faceted stones
- Fill the gallbladder
- Surgery is required
Symptoms of Gallstones
Asymptomatic gallstones (silent stones)
Most gallstones cause no symptoms. They are found incidentally on ultrasound performed for other reasons. 20-25% of asymptomatic gallstone carriers will develop symptoms within 10 years. Routine surgery for asymptomatic stones is not recommended in most patients - exceptions include diabetes, large stones (>3cm), non-functioning gallbladder, and some specific situations.
Biliary colic - classic symptomatic gallstone presentation
- Right upper abdominal pain starting 30-60 minutes after a fatty meal
- Cramping or colicky - waves of pain
- May radiate to right shoulder or right upper back
- Accompanied by nausea, sometimes vomiting
- Lasts 1-4 hours and then resolves completely
- Patient feels completely well between attacks
Biliary dyspepsia (atypical symptoms)
Some patients experience bloating, upper abdominal heaviness, and discomfort after fatty meals without classic severe colicky pain - biliary dyspepsia. This is caused by impaired gallbladder contraction against stones.
Causes and Risk Factors
- Female sex - oestrogen increases bile cholesterol saturation; pregnancy raises gallstone risk significantly
- Obesity and central adiposity - most important modifiable risk factor; increases biliary cholesterol secretion
- High-fat, low-fibre diet - typical of urban Indian dietary patterns
- Rapid weight loss - post-bariatric surgery causes gallstones in 30-40% of patients; bile becomes supersaturated during rapid fat mobilisation
- Diabetes mellitus - impairs gallbladder motility leading to bile stasis and stone formation
- Family history - genetic predisposition to cholesterol supersaturation in bile
- Haemolytic anaemia (sickle cell, thalassaemia) - excess bilirubin from red cell destruction forms pigment stones
- Prolonged fasting or TPN - gallbladder stasis without meals leads to sludge and stone formation
- Cirrhosis - impaired bile acid synthesis and secretion
Complications of Untreated Symptomatic Gallstones
| Complication | Mechanism | Management |
|---|---|---|
| Acute cholecystitis | Stone lodged at cystic duct → sustained obstruction → bacterial infection of gallbladder wall | IV antibiotics + laparoscopic cholecystectomy within 72 hours |
| CBD stones (Choledocholithiasis) | Stone migrates from gallbladder into common bile duct → bile duct obstruction | ERCP for stone removal → cholecystectomy |
| Cholangitis | CBD stone obstruction → bile stasis → bacterial infection of bile duct → sepsis | Emergency IV antibiotics + urgent ERCP |
| Gallstone pancreatitis | Stone impacted at ampulla → reflux of bile into pancreatic duct → pancreatic inflammation | IV fluids + pain control + cholecystectomy after recovery |
| Empyema gallbladder | Unresolved cholecystitis → pus filling gallbladder | Urgent cholecystectomy or cholecystostomy drainage |
| Gallbladder perforation | Pressure necrosis from stone obstruction → wall rupture → bile peritonitis | Emergency surgery |
Red Flags - Urgent Evaluation Needed
Seek urgent care if known gallstones are associated with:
- Fever - suggests cholecystitis or cholangitis
- Jaundice - suggests CBD stone obstruction
- Pain not resolving after 4-6 hours - cholecystitis developing
- Severe central pain radiating to back - pancreatitis
- Rapid deterioration - any of the above complications
Diagnosis
Ultrasound abdomen - gold standard
Identifies gallstones with >95% sensitivity in a fasted patient. Shows stone number, size, location, gallbladder wall thickness, and bile duct diameter. The first and most important investigation for suspected gallstone disease.
Blood tests
Liver function tests (elevated ALP, GGT, bilirubin if CBD stones), full blood count (raised WBC if infection), amylase/lipase (pancreatitis).
MRCP
Non-invasive bile duct imaging when CBD stones are suspected. Performed when ultrasound shows CBD dilatation or when liver function tests are abnormal.
CT scan
For complicated cholecystitis - identifies perforation, empyema, and pericholecystic collections.
Treatment of Gallstones
Asymptomatic gallstones
Observation is appropriate in most cases. Annual ultrasound to monitor. Prophylactic cholecystectomy is considered for: diabetic patients (higher complication risk), stones >3 cm (higher cancer risk), non-functioning gallbladder, porcelain gallbladder, incidentally discovered during other abdominal surgery.
Symptomatic gallstones - Laparoscopic cholecystectomy
Laparoscopic cholecystectomy (LC) is the definitive treatment for symptomatic gallstones. It is the gold standard worldwide and one of the most commonly performed operations in India. Key points:
- Performed through 3-4 small incisions (5-10mm) under general anaesthesia
- Takes 30-60 minutes in experienced hands
- Same-day or next-morning discharge in most patients
- Return to light activity in 5-7 days
- Full recovery in 2 weeks
- Major complication rate very low (<1%) in experienced laparoscopic surgeons
- Once the gallbladder is removed, biliary colic cannot recur
Non-surgical alternatives - limited role
Ursodeoxycholic acid (UDCA) dissolves small (<1 cm) cholesterol stones over 6-18 months - high recurrence after stopping. Not suitable for most patients. Surgery remains preferable for symptomatic stones.
Diet While Awaiting Surgery
- Avoid: All oily, fried, and fatty food - puri, bhajia, samosa, ghee-heavy curries, gathiya, chevdo, heavy festival meals. These trigger attacks.
- Choose: Plain dal, khichdi, soft roti without ghee, steamed vegetables, low-fat curd, fruit
- Remember: Diet manages symptoms but does not remove stones or prevent complications. Surgery provides the permanent solution.
Life After Cholecystectomy
- The gallbladder is not essential - bile drips continuously from the liver into the small intestine rather than being stored and released in boluses
- Most patients eat normally within 4-6 weeks including fatty food
- A small percentage (5-10%) experience post-cholecystectomy diarrhoea or loose stools from continuous bile entry - usually resolves within weeks; rarely requires treatment with cholestyramine
- No long-term dietary restriction is needed for most patients after full recovery
Frequently Asked Questions
Gallstones in India
India-specific context
- Gallstone disease is among the most common surgical conditions in India, with an estimated prevalence of 10-15% in the adult population and higher in certain regions including Gujarat, Rajasthan, and north India
- India has a disproportionately high burden of gallbladder cancer compared to Western countries - long-standing gallstone disease is the most important risk factor, making timely surgical management of symptomatic stones important from a cancer-prevention perspective
- The practice of managing symptomatic gallstones with antacids for months or years before seeking surgical care is extremely common in India - primarily due to misdiagnosis of biliary colic as acidity
- Post-bariatric cholecystectomy is increasingly relevant in India's growing bariatric surgical population - patients are screened and treated for gallstones developing after rapid weight loss
Desi Patient Questions
Jyaré symptoms aavya chhe (biliary colic even once) to surgery recommended chhe - recurrence expected chhe ane complications vadhé chhe time sathe. Asymptomatic stones generally observe thay chhe. Doctor sathe discuss karo - size, risk factors, ane symptoms based decision thay chhe.
4-6 weeks ma body adapt kare chhe. Majority patients normal diet resume kare chhe including fatty food. Thoda patients ne loose stools thay chhe initially - generally resolves. Long-term restriction most patients ne nathi padti. Normal Gujarati food including ghee reasonable quantities ma pachi khai shakay chhe.
Ha - laparoscopic cholecystectomy most commonly performed ane safest surgeries ma chhe India ma. 3-4 small holes (5-10mm), 30-60 minute, general anaesthesia. Same day ya next day discharge. 5-7 days light activity. Experienced surgeons ma major complications <1%. Dr Samir Contractor pase 8000+ laparoscopic surgeries experience chhe.
Seek Care in Vadodara
Gallstones confirmed on ultrasound - consult Dr Samir Contractor at Sterling Hospital, Vadodara for surgical assessment and laparoscopic cholecystectomy planning.
Gallstones Confirmed? Get a Surgical Consultation in Vadodara
Dr Samir Contractor at Sterling Hospital, Vadodara provides expert laparoscopic cholecystectomy with same-day discharge for most patients.