Gallstone pancreatitis occurs when a gallstone impacted at the junction of the bile duct and pancreatic duct triggers acute inflammation of the pancreas. It is the most common cause of acute pancreatitis in India. Severity ranges from mild and self-limiting to life-threatening. After recovery, cholecystectomy is essential to prevent the 30-50% recurrence rate within 6 weeks.
Quick Answers
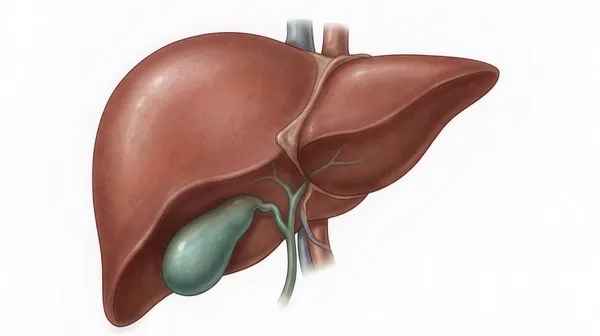
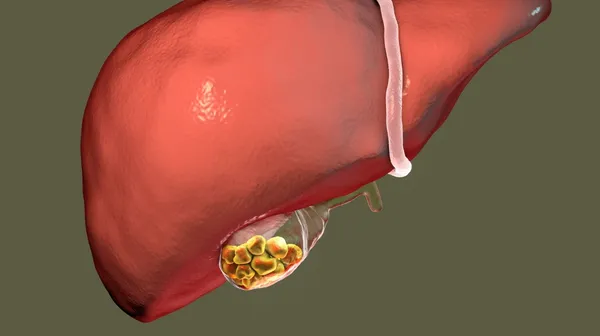
Gallstone pancreatitis is one of the most common and preventable serious GI emergencies in India. It occurs because the common bile duct and the pancreatic duct share a common channel (ampulla of Vater) before draining into the duodenum. When a gallstone impacts at this junction, bile refluxes into the pancreatic duct, activating pancreatic enzymes within the gland itself and causing autodigestion - acute pancreatitis.
Understanding why cholecystectomy after recovery is not optional - and why every episode of gallstone pancreatitis that goes untreated surgically risks a recurrence - is the critical message of this page.
Symptoms
- Severe, constant upper central abdominal pain - the hallmark; does not come and go; builds rapidly to maximum intensity
- Radiation to the back - classic; described as "boring through" to the back
- Worse lying flat - patients instinctively sit forward or curl up to reduce pain
- Nausea and persistent vomiting - vomiting does not relieve the pain (unlike some other abdominal conditions)
- Fever - may develop as inflammation progresses
- Jaundice - if the stone is still impacted at the ampulla
- Abdominal tenderness and distension
- Paralytic ileus - bowel sounds absent; no passage of stool or gas in severe cases
Severity Classification
Mild (80%)
- No organ failure
- No local complications
- Settles in 3-5 days
- IV fluids + pain control
- Cholecystectomy same admission
- Full recovery expected
Moderate (10-15%)
- Transient organ failure OR
- Local complications (fluid collections)
- Settles in 1-2 weeks
- HDU monitoring
- Cholecystectomy after recovery
- Generally good recovery
Severe (5-10%)
- Persistent organ failure
- Pancreatic necrosis
- ICU admission
- Significant mortality
- Specialist pancreatic centre needed
- Surgery/drainage for necrosis
80% of gallstone pancreatitis is mild and settles with IV fluids and supportive care within 3-5 days. The 20% with moderate-to-severe disease require intensive management. Cholecystectomy timing is adapted to severity - same admission for mild, after full recovery for severe.
Signs of severe pancreatitis needing intensive care:
- Falling blood pressure or rapid heart rate - shock from fluid sequestration
- Falling oxygen saturation - respiratory failure
- Declining kidney function - acute kidney injury
- Confusion - encephalopathy
- Worsening despite 48-72 hours of IV fluid resuscitation
- Fever with rising inflammatory markers - infected pancreatic necrosis
Diagnosis
- Blood tests: Serum amylase (>3 times upper limit of normal) or lipase (>3x) confirms pancreatitis; elevated liver function tests suggest gallstone cause; WBC elevated
- Ultrasound abdomen: Confirms gallstones; bile duct dilatation if CBD stone present; pancreatic oedema may be seen in mild disease
- CT scan abdomen (with contrast): Performed 48-72 hours after onset in moderate-severe pancreatitis to assess for pancreatic necrosis (non-enhancing areas on contrast CT)
- MRCP: When CBD stone is suspected in the clinical picture - non-invasive assessment before ERCP decision
Treatment
Acute management - for all severity grades
- Hospital admission - mandatory for all pancreatitis
- IV fluids - aggressive resuscitation (1-2 litres per hour initially for mild disease); the most important treatment for preventing complications
- Nil by mouth initially; then gradual diet reintroduction as pain settles
- IV pain control - analgesia titrated to severity
- Monitoring - vital signs, urine output, serial blood tests
ERCP - when indicated
ERCP is not routinely indicated for mild gallstone pancreatitis - the stone usually passes spontaneously. ERCP is indicated for: persisting CBD obstruction (persistent jaundice, dilated CBD); cholangitis developing on top of pancreatitis; or when CBD stones are confirmed on MRCP and symptoms are not settling.
Cholecystectomy - essential for prevention
Mild pancreatitis: Cholecystectectomy during the same hospitalisation, once pain and inflammatory markers have settled (typically day 3-5). Same-admission cholecystectomy prevents the 30-50% risk of recurrence within 6 weeks.
Moderate-severe pancreatitis: Defer cholecystectomy until full recovery (6-8 weeks) to allow pancreatic inflammation to settle fully before surgery.
Why Recurrence Is the Critical Risk Without Surgery
The 30-50% recurrence rate of gallstone pancreatitis within 6 weeks of a first episode is one of the most compelling arguments for same-admission cholecystectomy in mild disease. Recurrent pancreatitis episodes carry increasingly severe inflammation, higher complication rates, and greater mortality. Many patients who have their first mild pancreatitis episode - and are sent home without cholecystectomy - return with severe pancreatitis.
Same-admission cholecystectomy is the standard of care in guidelines from all major surgical societies. It is safe, effective, and prevents a significant preventable complication.
Frequently Asked Questions
Desi Patient Questions
Ha - absolutely zaruri chhe. Mild pancreatitis pachhi 30-50% patients 6 weeks ma pachi attack aavé chhe without surgery. Same admission cholecystectomy = most effective prevention. Recurrent pancreatitis episodes worse thay chhe. Doctor recommendation correct chhe - surgery avoid na karo.
Gallstone Pancreatitis? Get Admitted and Plan Same-Admission Surgery in Vadodara
Dr Samir Contractor at Sterling Hospital, Vadodara provides acute pancreatitis management and same-admission laparoscopic cholecystectomy to prevent recurrence.